





Field Staffing

2019
Medical staff in the MSF run intensive care unit (ICU) for critically ill COVID-19 patients, Al Gamhouria hospital Aden. (Photo credit: ©️Athmar Mohammed/MSF)

COVID-19 PANDEMIC
A year on and counting, the COVID-19 pandemic continues to ravage countries worldwide. Many are still experience supply issues of specific medical equipment to save patients' lives and keep frontline healthcare workers safe.
In most of the countries where MSF is responding, access to vaccines has been a major problem. In Palestine, only two percent of the population had been vaccinated by March 2021 and hospitals struggled to cope.
In Yemen, all aspects of the COVID-19 response are lacking and need greater international support, from public health messaging, to vaccinations, to oxygen therapy. While in India, which rode the first wave of COVID-19 relatively well, was overwhelmed by the second wave, which saw hundreds of thousands of people struggling to breathe and dying, many without receiving medical care.
Challenge: Staffing and supply chain impacted by disruption caused by COVID-19
Lockdown measures, travel restrictions, and a largely disrupted global transportation network posed major challenges to coordinating, staffing, and supplying MSF's global COVID-19 response in 2020. Where international travel was possible, medical and project staff departing for or returning from international missions faced extra layovers, long travel times, and lengthy testing and quarantine measures.
Global stockouts and shortages of essential protective and medical equipment, severely disrupted transportation networks, as well as temporary import and export restrictions on items needed for the COVID-19 response posed extraordinary supply and logistical challenges.

MSF supports Ji-Paraná's Municipal Hospital, in Rondônia state. Due to the pandemic's strain on the town's public health system, the hospital is now a COVID-19 referral center. (Photo credit: ©️Diego Baravelli)
Adaptation: Adapting to a new mode of care delivery
Despite these limitations, MSF continues to respond swiftly to the growing demands in many of our projects. With most commercial flights suspended for long periods, MSF staff relied largely on humanitarian charter flights to reach projects around the world. About 4,000 international staff travelled to MSF projects between April and December, only about 25% less than during the same period in 2019.
In some areas, our projects have been weakened, or we were forced to suspend our activities due to factors such as travel restrictions. Our locally-recruited staff, representing 90% of our employees in the field in our countries of intervention, have helped sustain our activities. We have also been able to adapt and innovate how we deliver care to maintain essential healthcare in our existing programmes amid this pandemic while accompanying ministries of health in preparing for or facing the pandemic.
From late February to the end of the year, MSF's supply centres packed close to 125 million items for the global COVID-19 response, including personal protective equipment, medical devices, medication, testing material, and specialised laboratory equipment, with another 162 million dispatched for regular and emergency projects.
COVID-19 training for the community in Indonesia. (Photo credit: ©️Cici Riesmasari/MSF)

.jpg)
2014
An MSF health worker in protective clothing carries a child suspected of having Ebola in the MSF treatment center on October 5, 2014 in Paynesville, Liberia. The girl and her mother, showing symptoms of the deadly disease, were awaiting test results for the virus. The Ebola epidemic has killed more than 3,400 people in West Africa, according to the World Health Organization. (Photo credit: ©️John Moore/Getting Images)
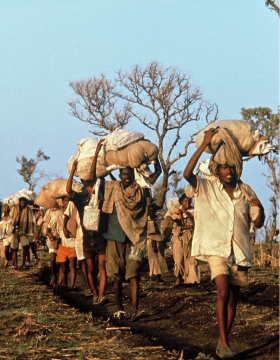
WEST AFRICA EBOLA OUTBREAK
The severity of the West Africa Ebola epidemic saw MSF launch one of the largest emergency operations in its history.
Between March 2014 and December 2015, MSF responded in the three most affected countries - Guinea, Liberia, and Sierra Leone – and also to the spread of cases to other countries affected by Ebola. MSF employed around 5,300 national staff and international staff who ran Ebola management centers as well as conducted surveillance, contact tracing, health promotion and provided psychological support. MSF admitted 10,310 patients to its Ebola management centers of which 5,201 were confirmed Ebola cases, representing 1/3 of all WHO-confirmed cases. During the first five months of the epidemic, MSF handled more than 85% of all hospitalised cases in the affected countries.
Challenge: Field staffing and emergency fund
The duration of frontline field assignments during this Ebola outbreak was much shorter than usual – at the height of the outbreak, assignments for international staff would last a maximum of six weeks. This was to ensure that staff remained alert and did not become too exhausted and then infected. This high turnover resulted in huge HR needs. Also, we had to draw on a small pool of field workers with highly specific skill sets required in an Ebola setting, especially at the beginning of the response. The few foreign governments that were willing to support mainly focused on funding or infrastructure but not staffing.
Given the huge challenge in staffing, nearly one-third of the emergency fund in the first year of the response was spent on staff costs, due to the huge HR needs in such a large response.
When the outbreak became out of control and spilled out of the continent, people began to be much more aware and pour in financial resources to support. In October 2014, MSF decided to launch a dedicated, earmarked fund for Ebola.

In the Ebola management center in Liberia, a washer is placing disinfected gloves of health workers for them to dry. (Photo credit: ©️Martin Zinggl/MSF)
Adaptation: HR Flexibility and Innovation
One of the ways to answer the problem was to try and mobilise even larger numbers of experienced international staff. The high levels of media interest in the Ebola crisis, MSF's response, and a strong dynamic in MSF's social networks, reinforced the global calls for more of those volunteers.
During the Ebola response, all other MSF programmes had to maintain their activities with fewer resources and support. With a very high level of unfilled positions, a new mobility policy was a concrete solution to decrease the pressure on HR.
More than 55 people relocated from their existing missions to the Ebola response. International positions were replaced by national staff, where they had the right experience and qualifications or where they could be reinforced through coaching and training.
MSF also decided to take the unusual step of training a large number of staff from other organisations. Because MSF was a leader in dealing with Ebola, we were able to transfer our knowledge to others. MSF also assisted WHO and the Centers for Disease Control (CDC) in developing their own training modules.
Health workers move an Ebola patient inside a MSF supported Ebola Treatment Centre (ETC) on July 09, 2014 in Sierra Leone. (Photo credit: ©️Sylvain Cherkaoui/Cosmos pour MSF)

